Quick Definitions
The following definitions provide a conceptual foundation for the terminology used throughout this discussion.
- GLP-1 (Glucagon-Like Peptide-1): An incretin hormone that promotes insulin secretion, suppresses glucagon release, slows gastric emptying, and influences appetite regulation.
- Tirzepatide: A synthetic peptide that activates both the GLP-1 and GIP receptors (dual incretin agonist). It coordinates hormonal signaling involved in insulin secretion, appetite regulation, and overall metabolic balance.
- GIP (Glucose-Dependent Insulinotropic Polypeptide): An incretin hormone involved in insulin secretion, adipose tissue signaling, and energy balance, with effects that vary by metabolic state.
- Dual agonist: A single ligand capable of activating more than one receptor class.
- Dual-incretin biology: Coordinated activation of both GLP-1 and GIP signaling pathways to influence metabolic regulation across multiple organ systems.
- Incretins: Hormones released from the gastrointestinal tract in response to nutrient intake that enhance glucose-dependent insulin secretion.
Introduction: From Single-Pathway Models to Integrated Metabolic Signaling
For much of the past two decades, incretin biology has been shaped by a largely reductionist framework. Glucagon-like peptide-1 (GLP-1) emerged as the dominant therapeutic target due to its well-characterized effects on glucose-dependent insulin secretion, appetite regulation, and gastrointestinal motility (Drucker, 2018).
Pharmacologic GLP-1 receptor agonists demonstrated that amplification of a single hormonal pathway could yield clinically meaningful improvements in glycemic control and body weight, reshaping therapeutic strategies for type 2 diabetes and obesity.
In contrast, glucose-dependent insulinotropic polypeptide (GIP) occupied a more ambiguous position. Early studies suggested that endogenous GIP responsiveness was diminished in insulin-resistant states, leading to the interpretation that GIP signaling was redundant or ineffective in metabolic disease (Nauck et al., 1993). As a result, incretin research remained largely GLP-1–centric for many years.
Tirzepatide emerged from a reassessment of these assumptions. Rather than viewing impaired endogenous GIP signaling as a limitation, investigators hypothesized that sustained pharmacologic activation of the GIP receptor, particularly when paired with GLP-1 receptor engagement, might reveal previously unrecognized aspects of incretin biology (Finan et al., 2016).
This shift reflected a broader evolution in metabolic science, moving away from single-pathway models toward an appreciation of metabolism as an integrated, network-driven system. Tirzepatide was therefore designed as a synthetic peptide capable of engaging both receptors within a single molecular framework. This design allowed investigators to examine whether coordinated incretin signaling could produce biological effects distinct from those achieved through mono-agonist strategies.
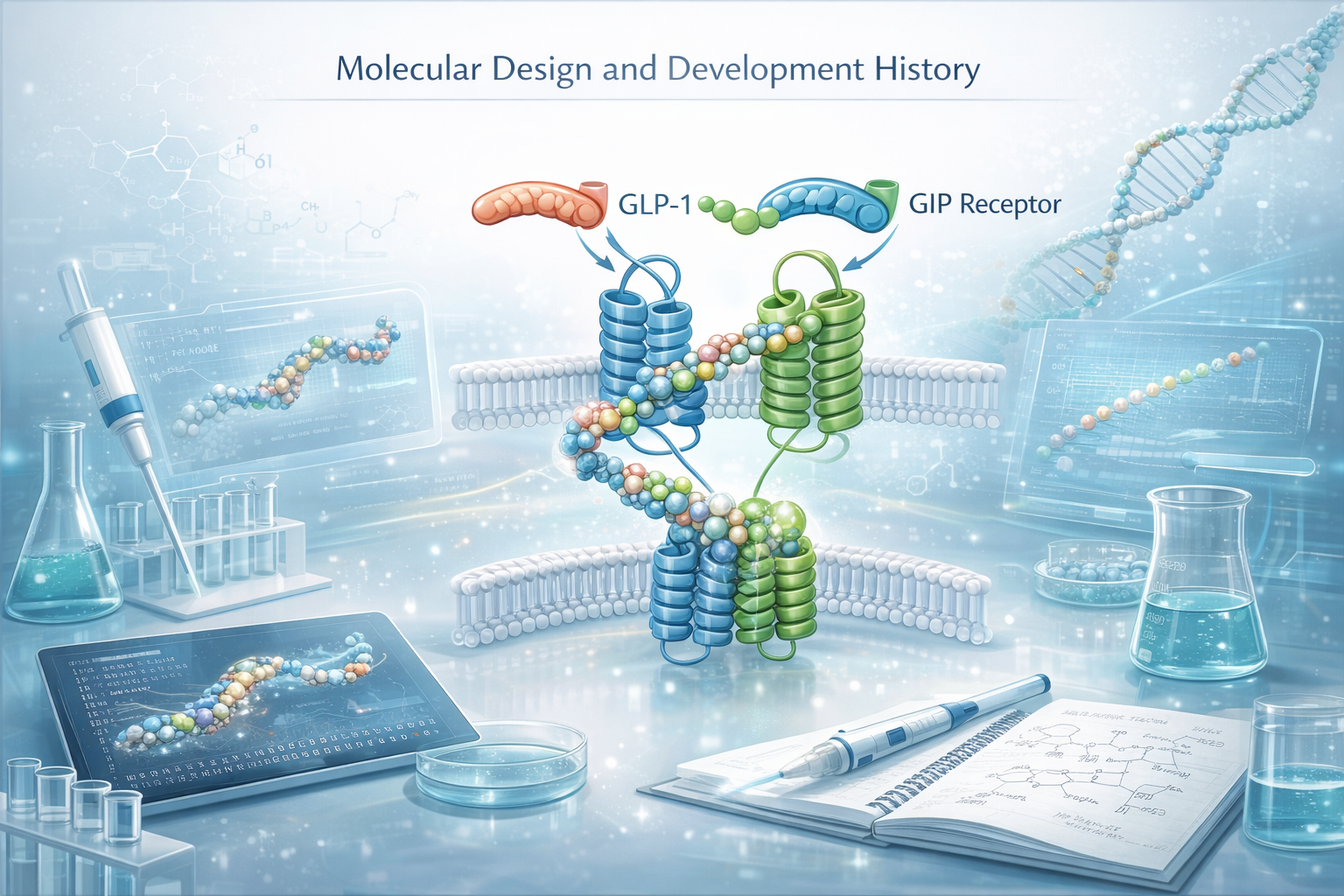
Molecular Design and Development History
Tirzepatide is a 39–amino acid synthetic peptide developed through rational peptide engineering and synthesized using solid-phase peptide synthesis. Its molecular architecture incorporates sequence elements that confer agonist activity at both the GIP and GLP-1 receptors, along with chemical modifications designed to enhance resistance to enzymatic degradation and prolong circulating half-life (Coskun et al., 2018).
These features enable sustained receptor engagement and make tirzepatide suitable for detailed pharmacologic investigation across experimental systems.
The conceptual foundations of tirzepatide trace back to early explorations of incretin physiology in the mid-2000s, when advances in peptide chemistry, receptor modeling, and structure–activity relationship analysis made it feasible to design multifunctional ligands with predictable receptor interactions.
Over time, interest shifted from asking whether GIP should be targeted at all to asking how GIP signaling might interact with GLP-1 signaling under conditions of sustained pharmacologic activation.
Tirzepatide progressed from in vitro receptor binding and signaling studies into animal models and, ultimately, large-scale human clinical trials (Coskun et al., 2018; Frias et al., 2018). As such, it reflects nearly two decades of cumulative research into incretin pathways and their role in metabolic homeostasis.
What Is Tirzepatide? Naming, Brand Names, and Regulatory Context
As tirzepatide transitioned from experimental compound to regulated pharmaceutical entity, distinctions between molecular identity and branded formulations became increasingly relevant.
Tirzepatide is the active pharmaceutical ingredient in two FDA-approved medications:
- Mounjaro®, approved for the treatment of type 2 diabetes mellitus
- Zepbound®, approved for chronic weight management in adults with obesity or overweight with weight-related comorbidities, and for obstructive sleep apnea in the context of obesity
Accordingly, tirzepatide refers to the molecular compound, while Mounjaro and Zepbound are branded formulations approved for specific regulatory indications. This distinction is particularly important when comparing tirzepatide to Wegovy®. Wegovy contains semaglutide, a GLP-1 receptor agonist that does not activate the GIP receptor (Coskun et al., 2018; Finan et al., 2016).
Brand names are referenced only to clarify terminology; this discussion is for research and educational purposes and does not constitute medical advice.
Why Dual-Incretin Biology?
Limitations of Mono-Agonist Models
Early incretin-based therapies focused almost exclusively on GLP-1 signaling, reflecting its established insulinotropic and anorectic effects. While effective, mono-agonist approaches implicitly assumed that other incretin pathways offered limited additive value in insulin-resistant states.
Emergent Properties of Coordinated Signaling
Subsequent research demonstrated that impaired endogenous GIP responsiveness does not preclude pharmacologic GIP receptor activation. When engaged with sufficient potency and duration, GIP signaling appears to interact with GLP-1 pathways in ways that influence insulin sensitivity, adipose tissue function, and central appetite regulation.
Dual-incretin biology therefore represents a shift from single-pathway amplification toward coordinated hormonal signaling. Rather than acting redundantly, GLP-1 and GIP receptor activation produces integrated metabolic effects that are not fully predictable from mono-agonist activity alone.
Dual Incretin Receptor Engagement: Mechanistic Foundations
Tirzepatide targets two class B G-protein–coupled receptors: the GIP receptor and the GLP-1 receptor. These receptors are expressed across multiple tissues involved in metabolic regulation, including pancreatic islet cells, the gastrointestinal tract, adipose tissue, and key regions of the central nervous system (Campbell & Drucker, 2013).
Activation of either receptor initiates cAMP-dependent signaling cascades, but downstream consequences vary by tissue and physiological context.
The defining mechanistic feature of tirzepatide is its simultaneous engagement of both receptors, creating an experimental platform for examining receptor synergy, dominance, and signaling bias.
Preclinical models suggest that dual receptor activation can reshape signaling responses in ways not predictable from single-receptor agonism, raising fundamental questions about whether incretin pathways operate independently or as interdependent components of a coordinated regulatory network (Finan et al., 2016).
Clinical Evidence Snapshot (High-Level)
Across randomized controlled trials in adults with type 2 diabetes and obesity, tirzepatide has demonstrated:
- Large, dose-dependent reductions in hemoglobin A1c
- Consistent reductions in body weight exceeding those observed with mono–GLP-1 receptor agonists
- Decreased caloric intake driven primarily by changes in appetite and satiety signaling
- Improvements in cardiometabolic risk markers, including blood pressure and lipid parameters
- Reductions in liver fat biomarkers and albuminuria in exploratory analyses
These findings reflect integrated metabolic effects observed under controlled clinical conditions and should be interpreted within the context of study design and duration.
Insights From Human Clinical Research
Human clinical trials constitute a central component of the tirzepatide research narrative. Across randomized controlled studies, tirzepatide produced large, dose-dependent reductions in hemoglobin A1c and body weight, consistently exceeding those observed with established mono-agonist GLP-1 therapies (Frias et al., 2021; Del Prato et al., 2021). These effects were sustained over the durations studied and observed across diverse patient populations.
Beyond glycemic measures, human research demonstrated marked reductions in caloric intake, alterations in appetite and satiety signaling, and improvements in insulin sensitivity (Heise et al., 2023). From a scientific standpoint, the importance of these trials lies not only in demonstrating efficacy but in illuminating the biological consequences of sustained dual receptor engagement in humans. The magnitude and consistency of observed responses suggest that incretin pathways interact in nonlinear ways involving coordinated contributions from peripheral tissues and central regulatory circuits.
System-Level Metabolic Effects and Tissue-Specific Responses
Human imaging and metabolic studies refined understanding of tirzepatide’s effects on body composition and tissue-specific metabolism. Weight loss associated with tirzepatide was driven predominantly by reductions in fat mass, with partial preservation of lean tissue (Heise et al., 2023).
This pattern raises important questions about how dual incretin signaling influences energy partitioning and tissue-specific nutrient utilization.
Reductions in liver fat content and improvements in hepatic biomarkers suggest relevance for metabolic-associated fatty liver disease, a condition closely linked to insulin resistance and visceral adiposity (Hartman et al., 2023).
Renal outcomes observed in clinical studies, including reductions in albuminuria and slower declines in estimated glomerular filtration rate, further suggest that the metabolic effects of tirzepatide may extend to organs traditionally viewed as secondary targets of metabolic disease (Heerspink et al., 2022). Whether these effects reflect direct receptor signaling, secondary consequences of weight loss, or a combination of both remains an active area of investigation.
Central Nervous System Involvement in Appetite and Energy Regulation
The central nervous system has emerged as a critical site of action in dual incretin biology. Human studies demonstrate that tirzepatide alters appetite regulation and food intake, consistent with engagement of hypothalamic and brainstem pathways involved in satiety and energy balance (Heise et al., 2023).
These findings reinforce the concept that metabolic disease cannot be fully understood through peripheral glucose handling alone, highlighting the importance of brain–gut–adipose communication in shaping energy intake and body weight.
Open Questions and Areas of Scientific Uncertainty
Despite extensive investigation, important questions remain unresolved. The relative contributions of direct receptor signaling versus secondary effects mediated by weight loss are not fully defined.
Long-term adaptive responses to chronic dual incretin stimulation, particularly beyond current trial durations, remain poorly characterized. Interindividual variability in response further raises questions about differences in receptor expression, signaling bias, and neural sensitivity across populations.
Future Directions in Dual-Agonist Research
Future research in incretin-based therapeutics is increasingly focused on extending dual-incretin frameworks toward multi-agonist signaling strategies.
The clinical and biological validation of tirzepatide has accelerated interest in peptides designed to engage additional metabolic receptors within a single molecular construct, reflecting a broader shift toward polypharmacologic approaches in metabolic science.
Among these next-generation compounds, retatrutide has emerged as a leading investigational example. Retatrutide is engineered to activate the GLP-1 receptor, the glucose-dependent insulinotropic polypeptide (GIP) receptor, and the glucagon receptor simultaneously.
The inclusion of glucagon receptor agonism is mechanistically motivated by its role in hepatic metabolism, lipid oxidation, and energy expenditure, complementing the insulinotropic and appetite-regulating effects mediated by GLP-1 and GIP signaling (Finan et al., 2015).
Preclinical studies demonstrated that coordinated activation of these three receptors could induce greater reductions in body weight and improvements in metabolic parameters than mono- or dual-agonist constructs, supporting translation into human investigation (Finan et al., 2015).
Early-phase clinical trials of retatrutide have provided proof-of-concept evidence that multi-agonist incretin therapies may further amplify metabolic effects observed with dual-incretin agonists under controlled study conditions (Jastreboff et al., 2023).
Importantly, the progression from mono-agonist to dual- and tri-agonist incretin therapies does not reflect a linear escalation of receptor effects. Rather, it underscores the increasingly recognized principle that metabolic regulation emerges from nonlinear interactions across hormonal, neural, and peripheral tissue signaling networks.
Within this continuum, tirzepatide functions as a reference molecule, informing both the scientific rationale and translational expectations for more complex multi-agonist designs (Finan et al., 2020).
“Tirzepatide reflects a shift from single-pathway models toward coordinated incretin signaling across integrated metabolic systems.”